
In the acute setting, our role is definitive treatment of those obvious chest pain patients, however not all patients need lysis or the cath lab, those that don't need these, need risk stratification.
In a perfect world everyone would be admitted, but we don't have that luxury. I made an estimate once that if we admitted every chest pain presentation to the hospital, our hospital beds would be full in no time at all.
When I think of chest pain, I think about the big 4:
In terms of missing fewer cases I always keep the following in mind:
In a perfect world everyone would be admitted, but we don't have that luxury. I made an estimate once that if we admitted every chest pain presentation to the hospital, our hospital beds would be full in no time at all.
When I think of chest pain, I think about the big 4:
- Ischaemia
- PE (refer to the module on Pulmonary Embolism)
- Dissection (refer to the module on Thoracic Aortic Dissection)
- Pneumothorax
In terms of missing fewer cases I always keep the following in mind:
- Textbooks presentations are only for those that spend their time in textbooks. Clinical medicine will fool you if you let it.
- The elderly always present atypically
- "If the patient sweats, you sweat"
- Shock is not always caused by infection( refer to the BP module)
- If the patient thinks they're going to die, they probably are. Listen ('angor animi', the Latin for impending doom.)
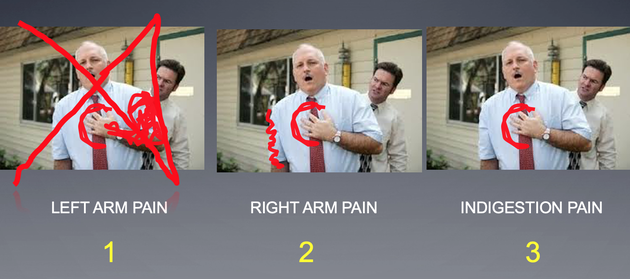
WHICH OF THESE HAS A HIGHER LIKELIHOOD RATIO OF PREDICTING MI?

ANSWER
Unfortunately that is not correct. The classic teaching of left arm radiation or pain has the lowest likelihood ratio of all three.
Try again.
Try again.
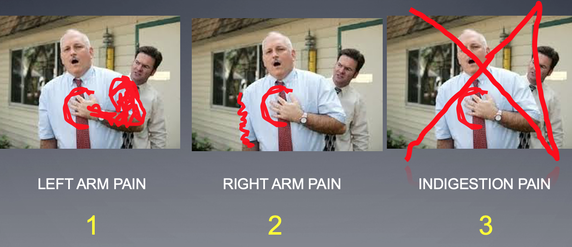
WINNER! It has the highest likelihood ratio of the three!

Indigestion pain has the second highest likelihood ratio of the three. Here's why we get caught out:
- About 8% of MI’s begin while eating
- In about 20% of cases, of MI, patient describes as ‘indigestion’
- About 50% of patients with AMI have increased belching with pain
- There is a higher incidence of GORD in patients with CAD

|
What about those patients that get better with a 'pink lady'?
(The pink lady is usually a concoction of malanga and xylocaine viscous.) In fact it is a POOR exclusion test. In a study in the Annals of Emerg Med (1995) it was shown that 15% of patients with an AMI get some relief and 7% get total relief. Don't rely own it as an exclusion test. |
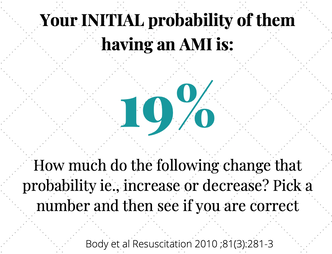
Case
A patient presents to the emergency department and your assessment of their probability for an AMI is 19%. How do the following affect that probability ie, does it increase or decrease and what number would you put on it?
|
THE PAIN IS:

answer
22%Surprised that it's only this much? |
THE PAIN IS:

answer
22% |
THE PATIENT HAS:

ANSWER
41%SURPRISED? |
THE PATIENT:

ANSWER
59% |
HOW DID YOU GO? WATCH WHAT THE AUDIENCE SAID AND DO A FEW MORE.
This is a fantastic video on symptoms and signs and how they affect our gestalt.
The TROPONIN
Troponin's have become so important in our approach to the chest pain patient in the emergency department. We use high sensitivity and we look at the delta value, so that even if the troponin is normal, if the delta is significant, we need to be concerned.
What is the delta, and how do we use it?
What about sex differences in troponin?
Do you use a point of care troponin in the ED?
Below are 4 videos from one of the worlds foremost experts on early rule out of low risk patients. Professor Louise Cullen. I have invited Louise to speak over the years and now we have a collection of what I think are the best Troponin lectures on the planet. WATCH THESE and enjoy the learning.
What is the delta, and how do we use it?
What about sex differences in troponin?
Do you use a point of care troponin in the ED?
Below are 4 videos from one of the worlds foremost experts on early rule out of low risk patients. Professor Louise Cullen. I have invited Louise to speak over the years and now we have a collection of what I think are the best Troponin lectures on the planet. WATCH THESE and enjoy the learning.
|
|
|
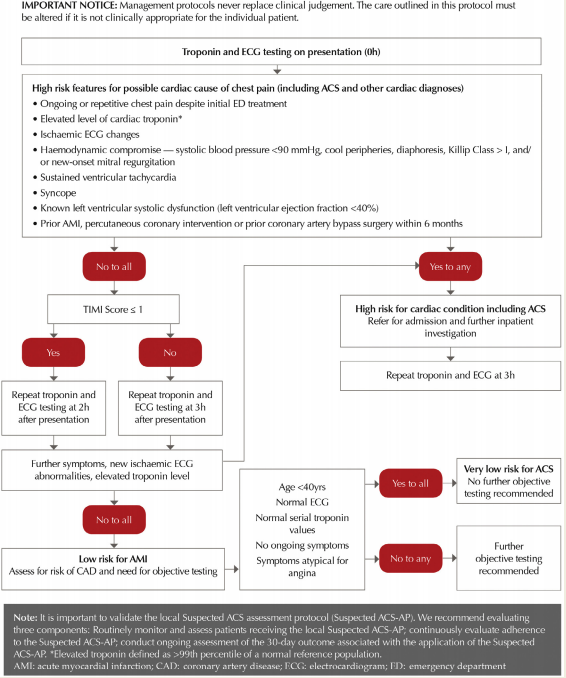
An example of a HIGH SENSITIVITY TROPONIN Approach from Australian and New Zealand Guidelines.
|
National Heart Foundation of Australia & Cardiac Society of Australia and New Zealand: Australian Clinical Guidelines for the Management of Acute Coronary Syndromes 2016. Heart, Lung and Circulation (2016) 25, 895–951 1443-9506/04/$36.00 http://dx.doi.org/10.1016/j.hlc.2016.06.789
|