
TAKE A MOMENT AND WRITE DOWN ALL THE CHANGES THAT MAY OCCUR IN THE ECG OF A PATIENT WITH PE.
ANSWER
There are about 10 ECG changes to know. We will go over some of these in this section
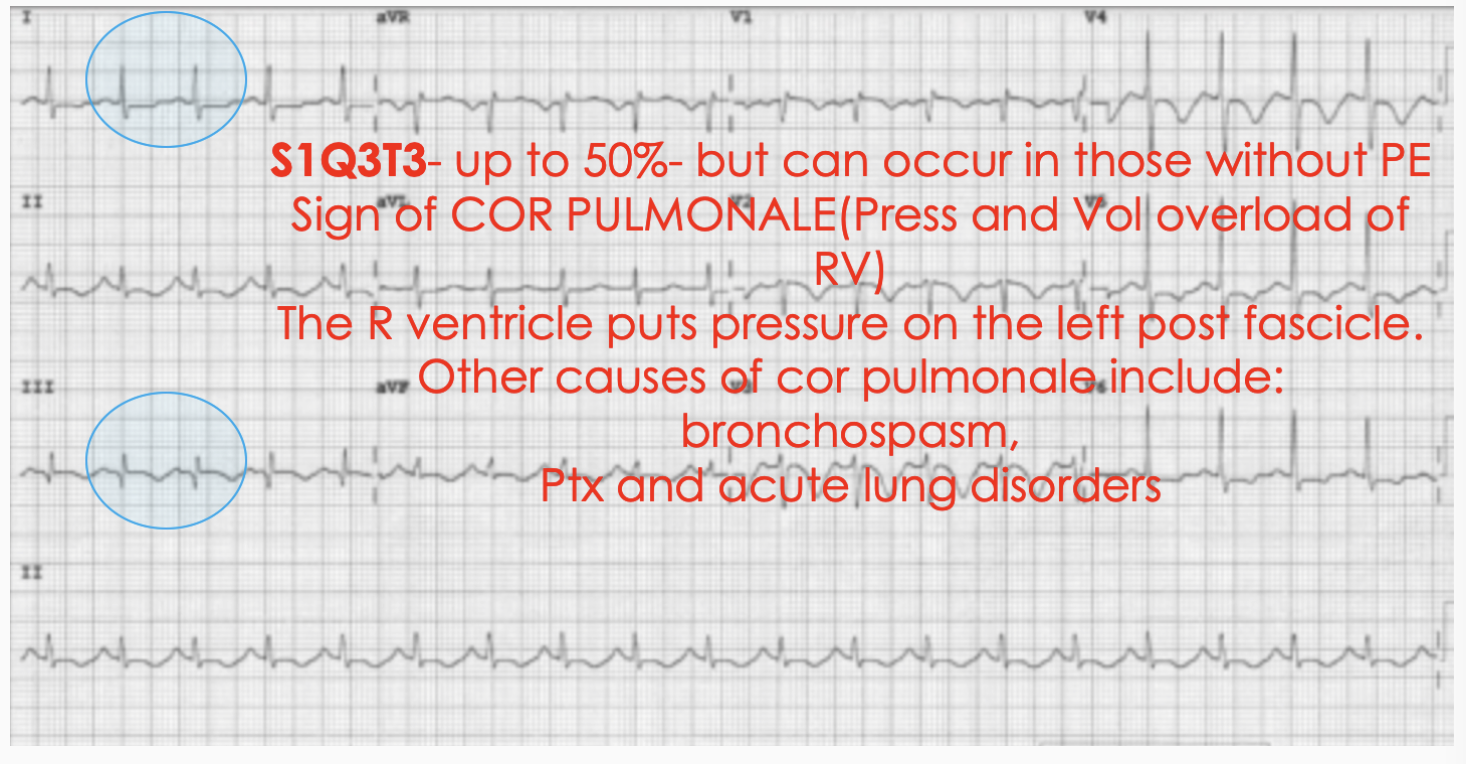
- S1Q3T3
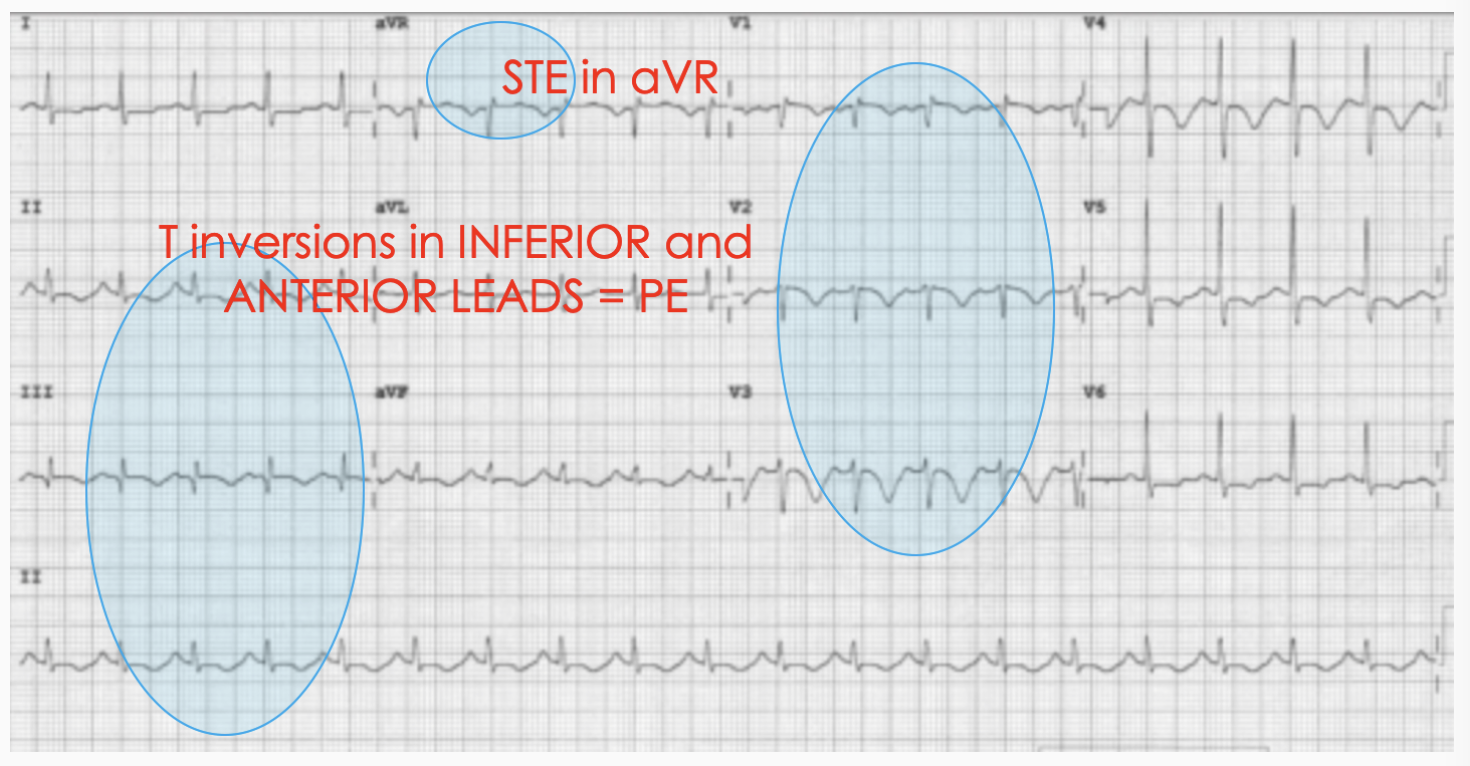
- T wave inversion in V1-V4
- ST elevation in aVR
- Bundle Branch Block: Complete or Incomplete
- Sinus Tachycardia
- Atrial Fibrillation
- P pulmonale
- Dominant R wave in V1
- Right Axis
- Transition point shift
What are the most ominous ECG Findings?
In a meta-analysis of 45 studies with 8209 patients, there were 6 ECG findings that predicted circulatory shock for pulmonary embolism. They showed right ventricular strain from acute pulmonary hypertension and were associated with significantly increased probability of circulatory shock and death from PE.
From the 10 changes we identified in the question above, can you pick which 6 were the most important?
From the 10 changes we identified in the question above, can you pick which 6 were the most important?
ANSWER
1. Sinus Tachycardia
2. Atrial Fibrillation
3. S1Q3T3
4. RBBB
5. T wave inversion in V2-V3
6. ST Elevation in aVR
2. Atrial Fibrillation
3. S1Q3T3
4. RBBB
5. T wave inversion in V2-V3
6. ST Elevation in aVR
In a recent study that looked at ECG findings prior to the patient deteriorating into a PEA or asystolic arrest, it was found that the most common terminal morphology(67% of cases) was a RBBB in V1, which progressed from an increasing RV delay as shown below:

Definite Right Ventricular strain(RVS) pattern was defined as having the above progressive morphological changes in lead V1 and either no intraventricular conduction delay or terminal intraventricular conduction delay (ie., incomplete RBBB) and two or more of the following occurring simultaneously:
- ST elevation V1
- Rightward directed ST elevation vector in limb leads (i.e. towards lead III) or
- Right axis deviation in limb leads
It's also important to differentiate between PE and ischaemia
Kosuge M et al looked 40 patietnets with PE and 87 patients with acute coronary syndrome. They found that NEGATIVE T waves in III and V1 had a 97% positive predictive value for PE.
Kosuge M et al AJJ 99:15 March 2007;pp817-821 Electrocardiographic Differentiation Between Acute Pulmonary Embolism and Acute Coronary Syndromes on the Basis of Negative T waves.
Kosuge M et al AJJ 99:15 March 2007;pp817-821 Electrocardiographic Differentiation Between Acute Pulmonary Embolism and Acute Coronary Syndromes on the Basis of Negative T waves.
CASE 1
A 71 yo male presents with central crushing chest pain and dyspnoea at rest.
His past medical history includes:
What changes do you see on this ECG and what might they mean, based on the previous sections?
Write down the changes that might be consistent with ischaemia and those that might be consistent with a pulmonary embolism..
A 71 yo male presents with central crushing chest pain and dyspnoea at rest.
His past medical history includes:
- Hypercholesterolaemia
- Smoking
- A hip replacement one month previously. He has been on Clexane until 3 days ago.
What changes do you see on this ECG and what might they mean, based on the previous sections?
Write down the changes that might be consistent with ischaemia and those that might be consistent with a pulmonary embolism..
In this case(taken from the literature) the ECG changes were seen to be consistent with ischaemia.
A troponin was done and it was raised.
The patient was treated with Aspirin/LMWH and IIB/IIIA inhibitors.
The patient became haemodynamically unstable and was taken to the cath lab. It was found that he had normal coronary vessels, but a complete occlusion of the tight pulmonary artery.
This is a great case to learn from.
What are the ECG changes you found that might be consistent with a Pulmonary Embolism? Click below for the answer.
A troponin was done and it was raised.
The patient was treated with Aspirin/LMWH and IIB/IIIA inhibitors.
The patient became haemodynamically unstable and was taken to the cath lab. It was found that he had normal coronary vessels, but a complete occlusion of the tight pulmonary artery.
This is a great case to learn from.
What are the ECG changes you found that might be consistent with a Pulmonary Embolism? Click below for the answer.
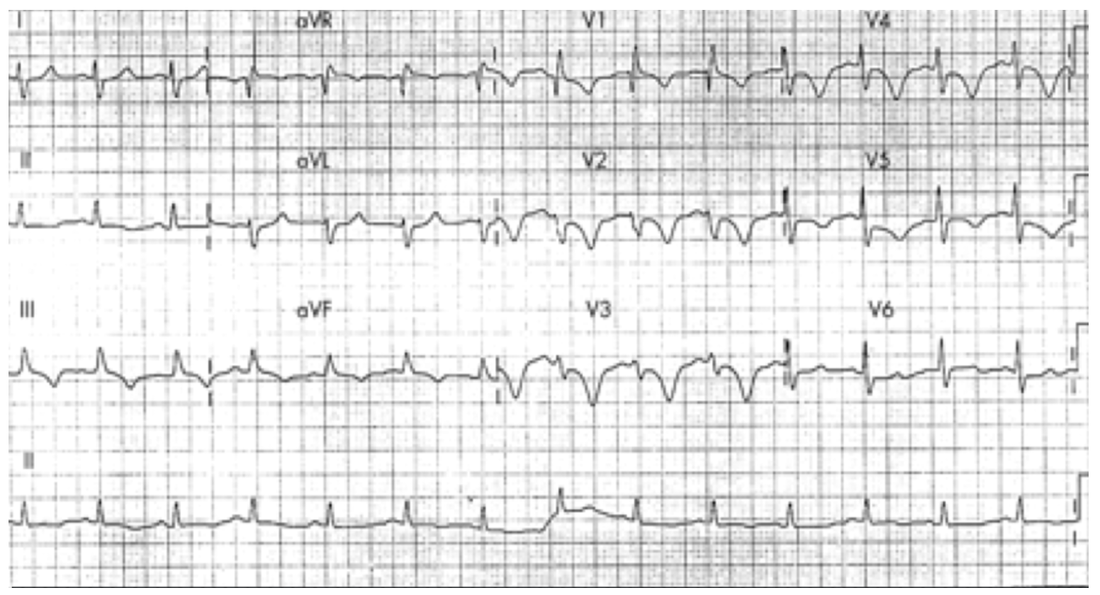
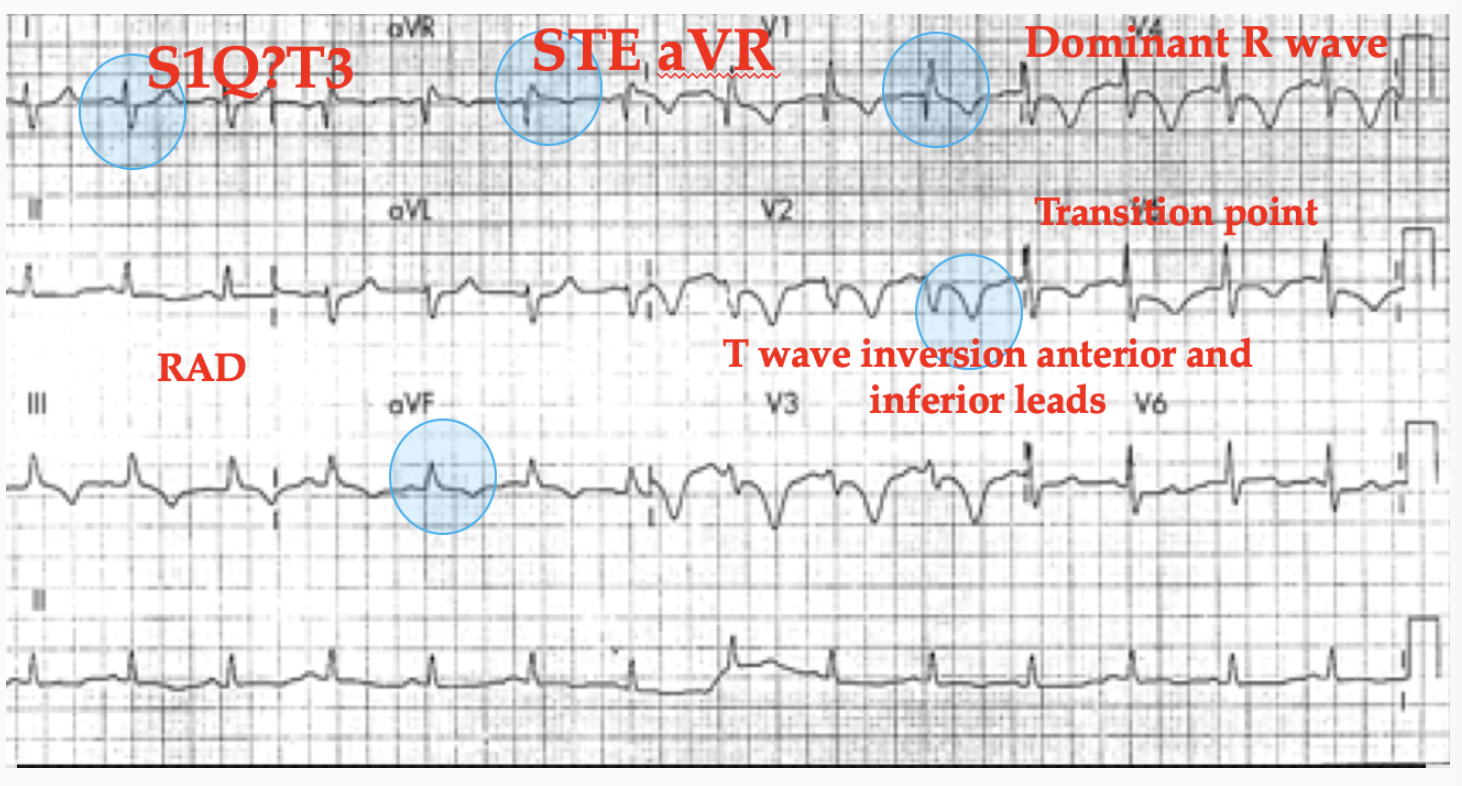
ECG ANSWER TO 71 YO MALE PRESENTING WITH CENTRAL CRUSHING CHEST PAIN AND DYSPNOEA
We see that the ECG below has some of the findings we described above. Although no clear S1Q3T3, there are 5 other signs.
Case 2
An 85 yo woman presents with a sudden increased shortness of breath.
Past medical history includes breast malignancy
Her vitals are: HR 156, Resp rate 28, Sats 88% on room air
On examination, she has a clear chest and her chest xray is normal.
Her ECG is shown below:
What does the ECG show? Take a moment to answer this.
The question to be answered here is why are her saturations low, given a clear chest and a clear chest xray? In these cases we must always think of a pulmonary embolism.
Past medical history includes breast malignancy
Her vitals are: HR 156, Resp rate 28, Sats 88% on room air
On examination, she has a clear chest and her chest xray is normal.
Her ECG is shown below:
What does the ECG show? Take a moment to answer this.
The question to be answered here is why are her saturations low, given a clear chest and a clear chest xray? In these cases we must always think of a pulmonary embolism.
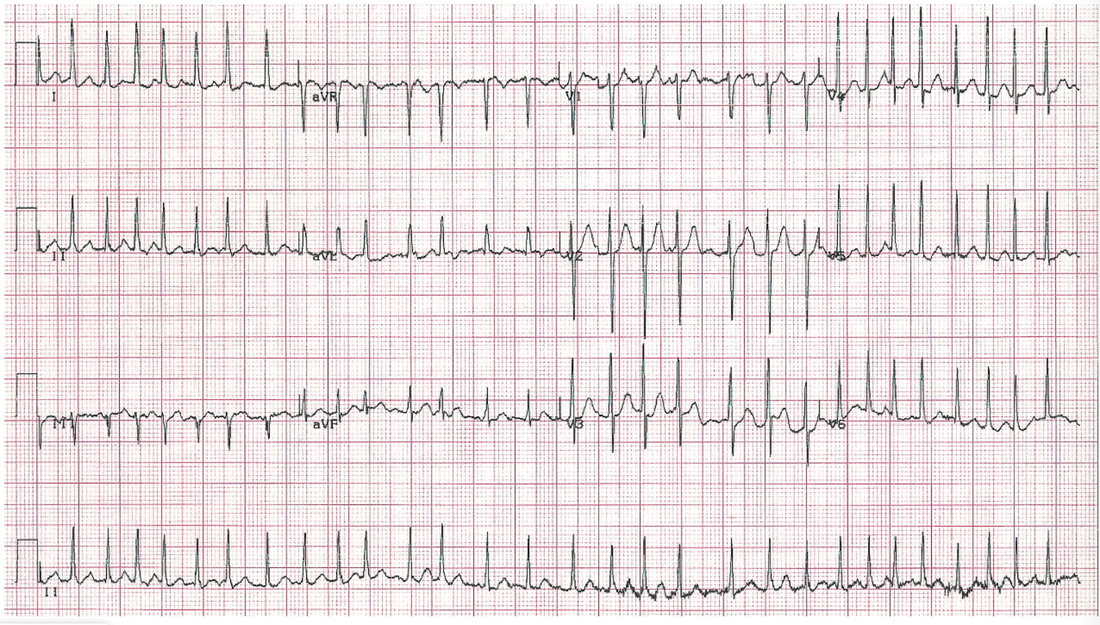
This is a tachycardia, and it is a new atrial fibrillation. That may be all we need.
Case 3
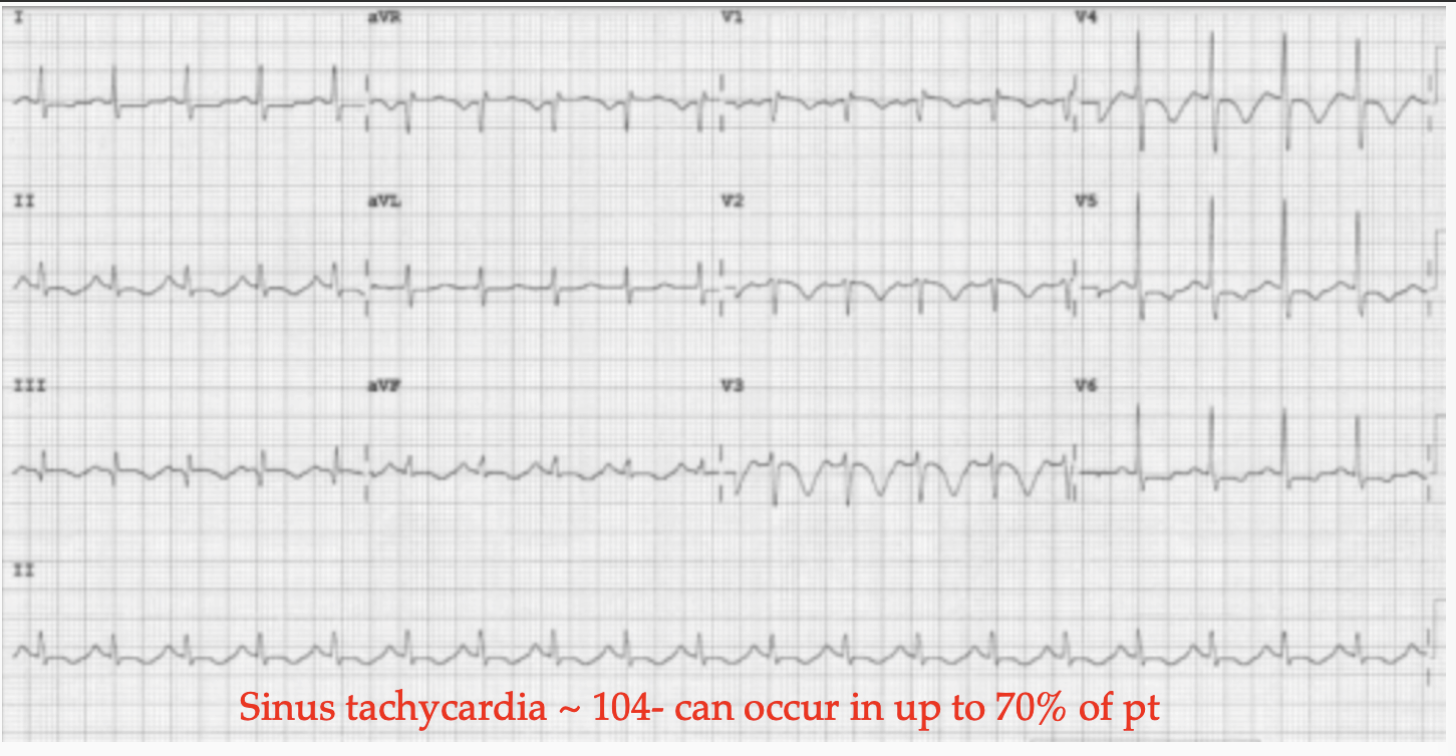
A 68 yo woman presents with worsening dyspnoea. What is her diagnosis?
Write down what you see on the ECG.
Write down what you see on the ECG.

ANSWER TO 68 YO WOMAN WITH DYSPNOEA
Scoring Systems
DO ANY OF THE SCORING SYSTEMS FOR DIAGNOSING PE INCLUDE THE ECG?
There are no specific ECG finding in the Wells or the Geneva scores or even the PERC rule. However they do include a measurement of HEART RATE.
Are the ECG Scoring Systems?
Just like the condition of pulmonary embolism has various scoring systems to help with making the diagnosis, so do ECGs. However the scoring systems related to ECGs are mostly about the severity of disease. When you fit one of these systems, the condition is very severe. Here is one such scoring systems.
There are no specific ECG finding in the Wells or the Geneva scores or even the PERC rule. However they do include a measurement of HEART RATE.
Are the ECG Scoring Systems?
Just like the condition of pulmonary embolism has various scoring systems to help with making the diagnosis, so do ECGs. However the scoring systems related to ECGs are mostly about the severity of disease. When you fit one of these systems, the condition is very severe. Here is one such scoring systems.
The Daniel Score |
Daniel K R et al. Assessment of Cardiac Stress from Massive Pulmonary Embolism with 12-lead ECG.
Chest 2001, Aug;120(2):474-81 |
A score > 10 indicates severe pulmonary hypertension
- Sinus Tachycardia(2 points)
- RBBB(incomplete)(2 points)
- RBBB(complete)(3 points)
- T wave inversion V1-V4(0-12 points)
- S wave in I(0 points)
- Q wave in III(1 point)
- Inverted T wave in III(1 point)
- S1Q3T3(2 points)