
THORACIC AORTIC DISSECTION
|
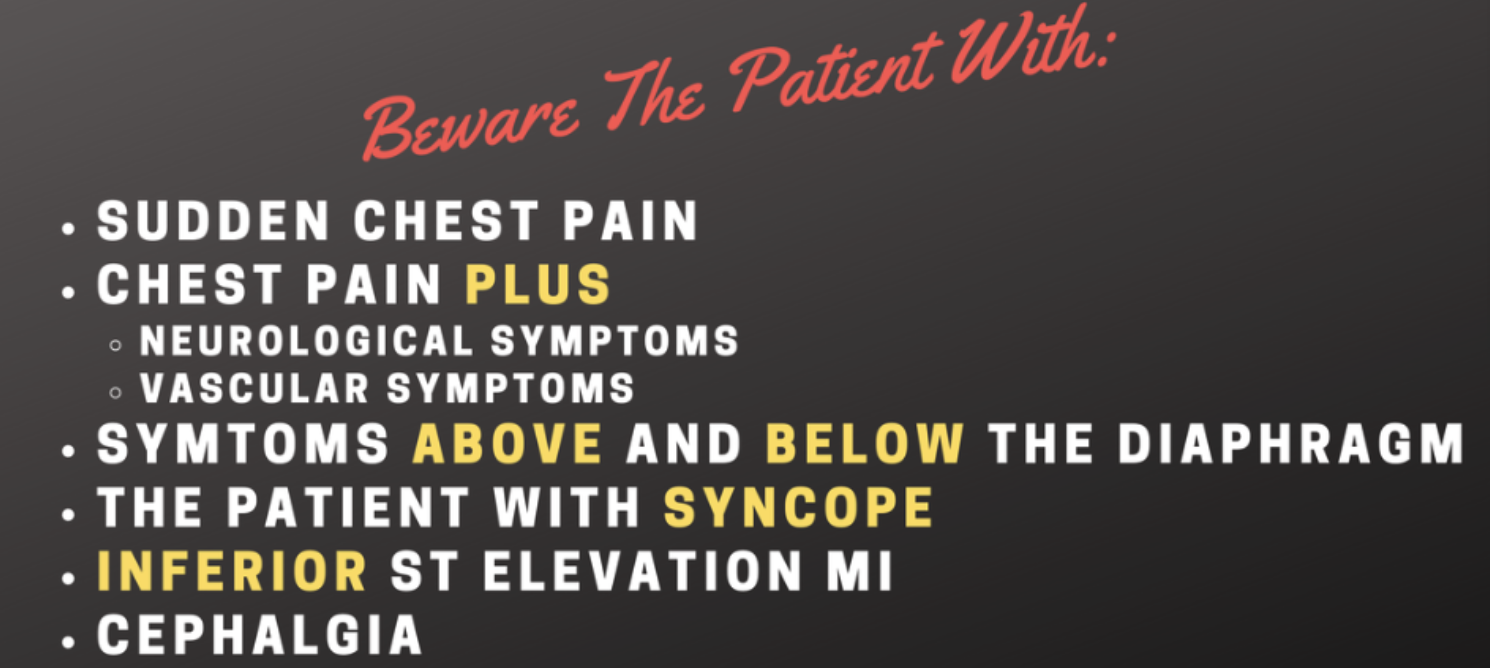
Here are some risk factors you may, or may not have thought of:
|
Chest X-ray Findings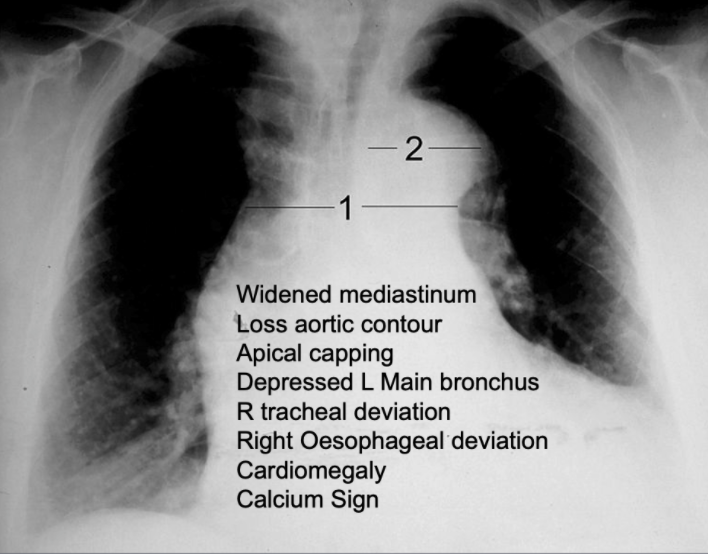
|
Remember the following to maximise pickups.
|
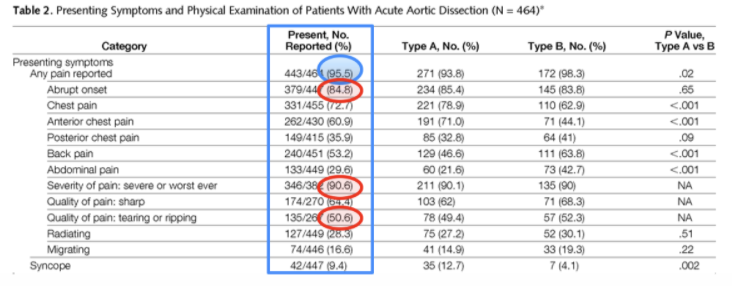
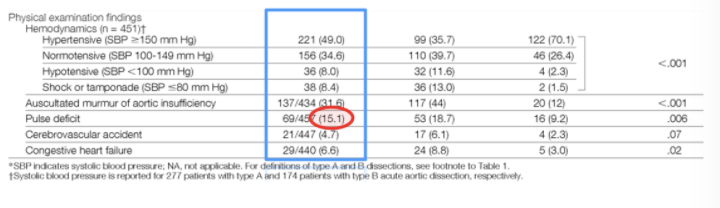
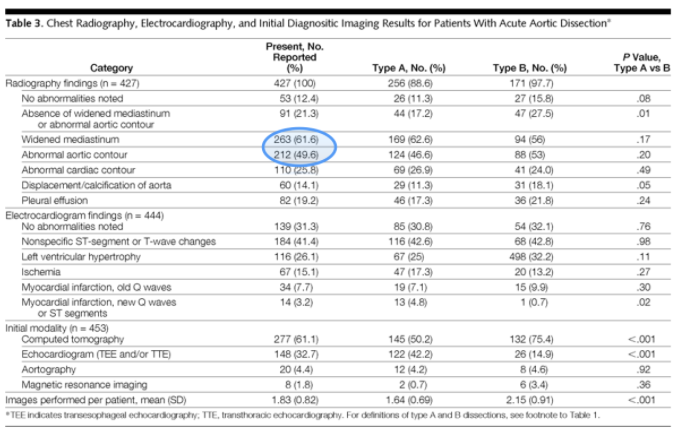
What Are The Important Symptoms? Write down 3.Perhaps the best reference for this is the IRAD Study.
Hagan, p et al The International Registry of Acute Aortic Dissection(IRAD) New Insights into an old disease. JAMA.2000;283 89-903. PAIN Abrupt onset and severe pain are significant findings. Interestingly the 'tearing' quality of the pain that we have heard of in the textbooks is present in only about 50% of the patients. PHYSICAL FINDINGS The classic teaching of a 'pulse deficit', is shown not to be present frequently. However nearly 50% of patients are hypertensive. RADIOGRAPHIC FINDINGS The classic teaching of the widened mediastinum on the chest xray is not as common as we think. A widened mediastinum was found to be present in about 62% of cases and an abnormal aortic contour is only present in about 50% of cases. |
|
Some of the Clinical Presentations
PAIN
A 56 yo male has presented with sudden severe central chest pain that has moved over his shoulders and into his back.
Beware this movement of pain. It can occur as the dissection progresses:
PERIPHERAL ARTERY DISSECTIONMALPERFUSION SYNDROME
AS VESSELS DISSECT THE MALPERFUSION CAN PRESENT AS:
A 56 yo male presents to the emergency department. He has central severe chest pain that started abruptly and now continues and he is diaphoretic.
His ECG is shown below. What do you think.
PAIN
A 56 yo male has presented with sudden severe central chest pain that has moved over his shoulders and into his back.
Beware this movement of pain. It can occur as the dissection progresses:
- Ascending aorta: anterior chest wall pain
- Descending Aorta: Pain moves into the upper back
- Lower dissection: Pain moves into the lower back.
PERIPHERAL ARTERY DISSECTIONMALPERFUSION SYNDROME
AS VESSELS DISSECT THE MALPERFUSION CAN PRESENT AS:
- Carotid Artery Territory:
- This can present as Stroke
- It can also present as sudden severe headache ie., subarachnoid Haemorrhage.
- Renal Artery: Renal Failure
- Artery of Adamkiewicz : Leg Weakness and paraplegia
- Superior Mesenteric Artery: Bowel Ischaemia
- Coronary Vessels: Myocardial Infarction
A 56 yo male presents to the emergency department. He has central severe chest pain that started abruptly and now continues and he is diaphoretic.
His ECG is shown below. What do you think.
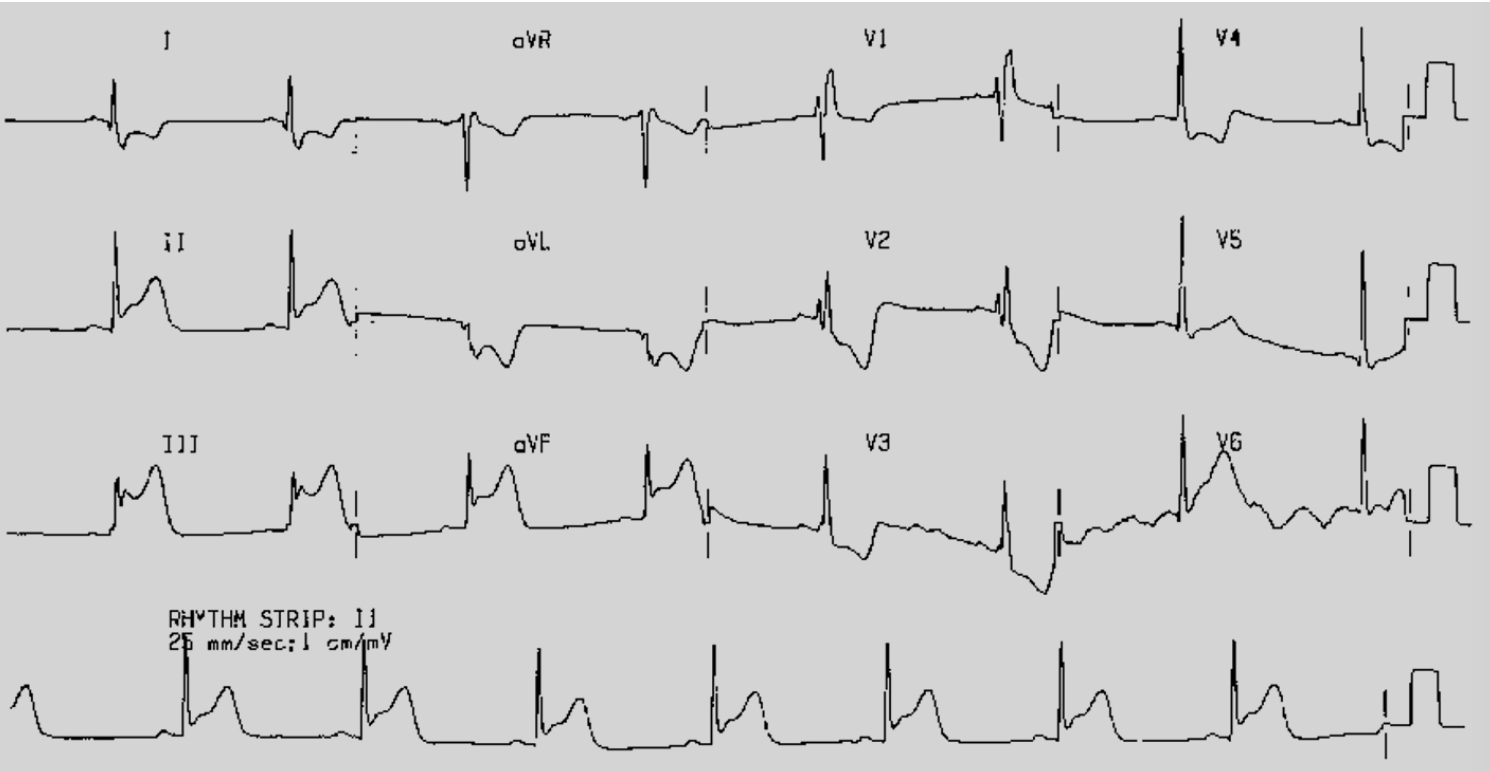
ECG INTERPRETATION:
There is a right bundle branch block.
There is ST elevation in the inferior leads II, III and aVF, with STE in III>II
There is reciprocal ST depression in leads I and aVL as well as in leads V1-V4
In Conclusion: There is an INFERIOR ST Elevation MI, with possible posterior and Right Ventricular infarction. Right Ventricular leads need to be done.
In this particular case, with the story involved, there may be a thoracic aortic dissection with Right Coronary Artery Dissection.
We need a Chest Xray on this patient.
He needs that and discussion with cardiology before any thrombolysis is given, if there is no cath lab.
There is ST elevation in the inferior leads II, III and aVF, with STE in III>II
There is reciprocal ST depression in leads I and aVL as well as in leads V1-V4
In Conclusion: There is an INFERIOR ST Elevation MI, with possible posterior and Right Ventricular infarction. Right Ventricular leads need to be done.
In this particular case, with the story involved, there may be a thoracic aortic dissection with Right Coronary Artery Dissection.
We need a Chest Xray on this patient.
He needs that and discussion with cardiology before any thrombolysis is given, if there is no cath lab.
outcome of this case
A diagnosis of myocardial infarction was made. No Chest Xray was performed and the patient received thrombolytics.
The patient decompensated. An ECHO demonstrated a pericardial effusion. There was an underlying thoracic aortic dissection. The patient arrested and could not be resuscitated.
This was a very famous case in the US as it involved a well known sitcom actor.
The patient decompensated. An ECHO demonstrated a pericardial effusion. There was an underlying thoracic aortic dissection. The patient arrested and could not be resuscitated.
This was a very famous case in the US as it involved a well known sitcom actor.
Watch Thoracic Aortic Dissection