
VENTRICULAR BIGEMINY
A 62 year old patient presents to your emergency department with palpitations.
Her rhythm strip is shown below:
What is the diagnosis?
Is this a benign rhythm?
Her rhythm strip is shown below:
What is the diagnosis?
Is this a benign rhythm?

ANSWER
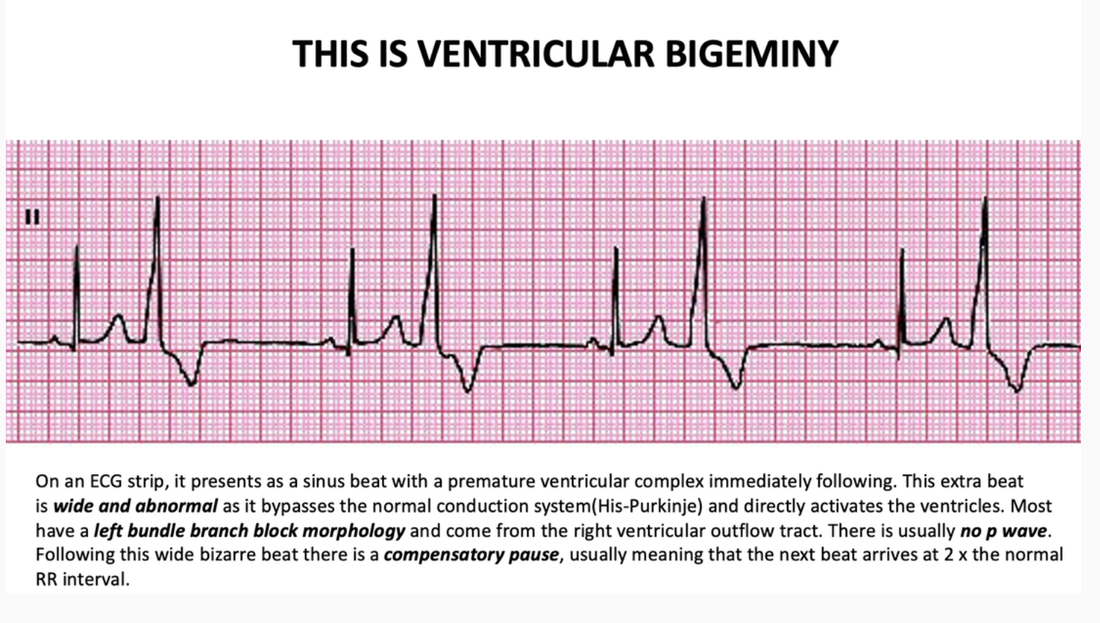
Bigeminy comes for the latin for ‘twins’. On an ECG strip, it presents as a sinus beat with a premature ventricular complex immediately following. This extra beat is wide and abnormal as it bypasses the normal conduction system(His-Purkinje) and directly activates the ventricles. Most have a left bundle branch block morphology and come from the right ventricular outflow tract. There is usually no p wave. Following this wide bizarre beat there is a compensatory pause, usually meaning that the next beat arrives at 2 x the normal RR interval.
TERMINOLOGY/CLASSIFICATIONVentricular Bigeminy = A ectopic beat every second beat
Ventricular Trigeminy = An ectopic beat every third bead
Ventricular Quadrigeminy = An ectopic beat every fourth beat.
Ectopic beats can be both ventricular and atrial. In atrial bigeminy, each normal beat is followed by a premature beat.
Classification can be according to the frequency; i.e.., > 10/hr or 6/minute are very frequent, or to their clinical significance; i.e.., benign or potentially malignant. Formal classifications such as the Lown classification are not frequently used.
WHAT CAUSES THEM?
HOW IMPORTANT ARE THEY?We normally don’t need to do anything for these patients, as ectopics are a normal physiological response. However:
INVESTIGATIONSThese are straightforward:
MANAGEMENTIn asymptomatic patients with an incidental finding, do nothing. Give advice on coffee consumption, energy drinks etc.
In symptomatic patients:
If Normal left ventricular function and no known coronary artery disease:
TERMINOLOGY/CLASSIFICATIONVentricular Bigeminy = A ectopic beat every second beat
Ventricular Trigeminy = An ectopic beat every third bead
Ventricular Quadrigeminy = An ectopic beat every fourth beat.
Ectopic beats can be both ventricular and atrial. In atrial bigeminy, each normal beat is followed by a premature beat.
Classification can be according to the frequency; i.e.., > 10/hr or 6/minute are very frequent, or to their clinical significance; i.e.., benign or potentially malignant. Formal classifications such as the Lown classification are not frequently used.
WHAT CAUSES THEM?
- Sympathetic drivers such as ; anxiety, caffeine
- beta agonists
- hypokalaemia
- hypomanesaemia
- Digoxin toxicity
- Ischaemia ( this is an important cause not to forget)
HOW IMPORTANT ARE THEY?We normally don’t need to do anything for these patients, as ectopics are a normal physiological response. However:
- In patients with ischaemic heart disease, these may be significant and caused by the ischaemia. Beware the multiple premature ventricular ectopics in MI.
- Beware premature ventricular contractions(PVC’s) and Long QTc as this may predispose to R on T phenomenon. The premature complex may fall on the T wave resulting in Torsades de Pointes.
INVESTIGATIONSThese are straightforward:
- Look for electrolyte disturbances.
- Perform a troponin, in case there is ischaemia.
- In patients being discharged, an exercise stress test may be appropriate as it may show increased PVC’s with ischaemia.
- An ECHO specifically looking at left ventricular function is important as, there is increased risk in those with an ejection fraction < 40%
MANAGEMENTIn asymptomatic patients with an incidental finding, do nothing. Give advice on coffee consumption, energy drinks etc.
In symptomatic patients:
If Normal left ventricular function and no known coronary artery disease:
- Consider a beta blocker such as Metoprolol
- Invasive strategies may be needed if > 2 of the following are present:
- LVEF < 40%
- Ventricular late potentials
- Repetitive VPC’s