
MONOMORPHIC and POLYMORPHIC VENTRICULAR TACHYCARDIA
MONOMORPHIC VENTRICULAR TACHYCARDIA
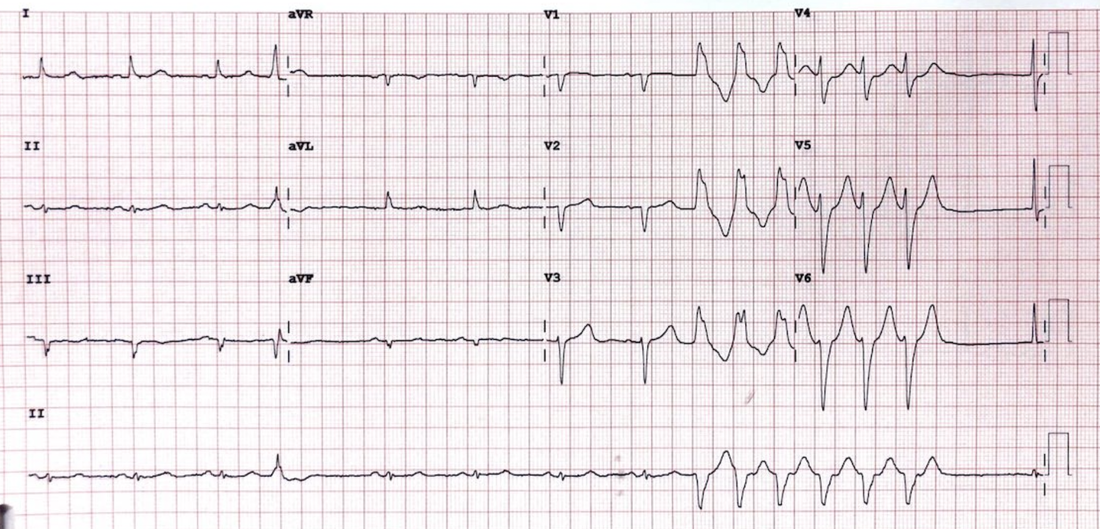
This is a regular wide complex tachycardia, that originates from a single focus in the ventricle.
It can be either sustained or not-sustained. Non-sustained is defined as self terminating and not lasting for more than 3 complexes or 30 seconds. Below is an example of non-sustained monomorphic ventricular tachycardia.
This is a regular wide complex tachycardia, that originates from a single focus in the ventricle.
It can be either sustained or not-sustained. Non-sustained is defined as self terminating and not lasting for more than 3 complexes or 30 seconds. Below is an example of non-sustained monomorphic ventricular tachycardia.
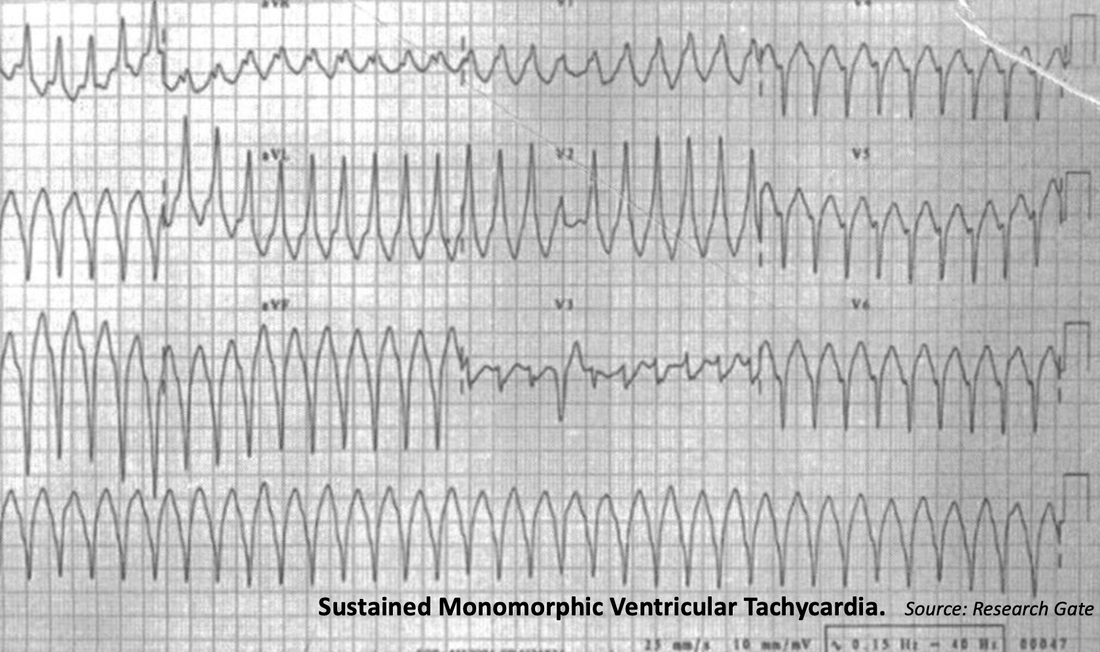
Below is an example of sustained monomorphic ventricular tachycardia with a right bundle branch morphology.
To see how to diagnose VT go to the Ventricular tachycardia section of the course.
To see how to diagnose VT go to the Ventricular tachycardia section of the course.
Causes of Monomorphic Ventricular Tachycardia
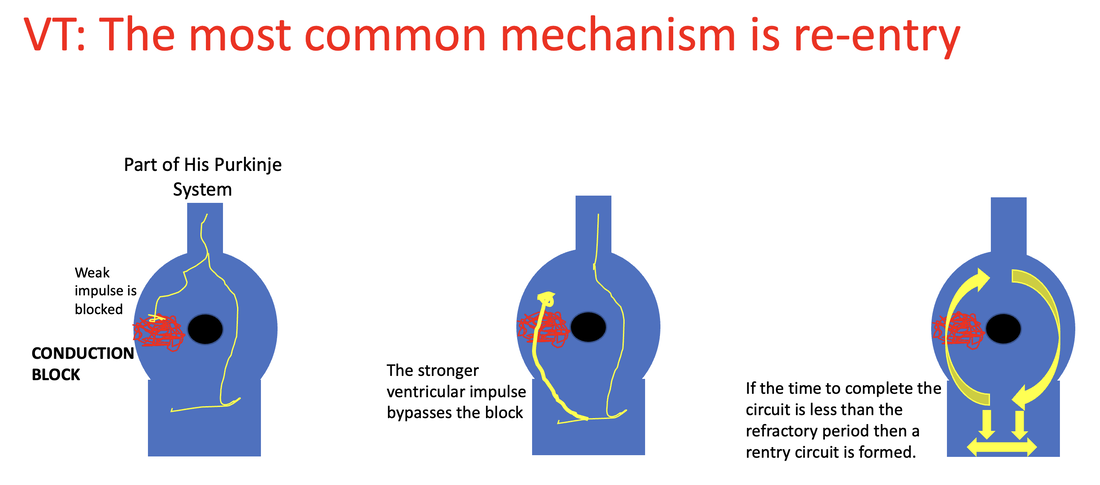
It is usually due to reentry through regions of myocardial scar that promote slow conduction pathways and create the conditions for reentry as shown below.
- Structural Heart Disease is the most likely cause
- This can include non-ischaemic cardiomyopathy
- It can also be in scar tissue post a previous myocardial infarction
- Not usually due to acute ischaemia
It is usually due to reentry through regions of myocardial scar that promote slow conduction pathways and create the conditions for reentry as shown below.
|
Monomorphic VT is usually not associated with ischaemia.
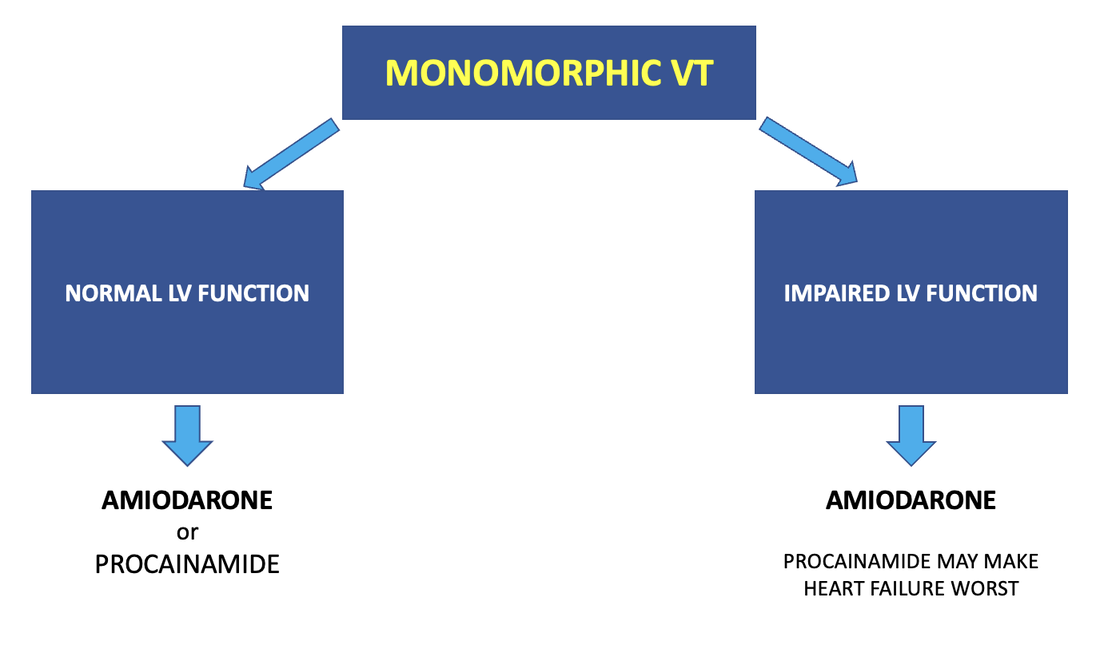
Treatment Electrical Cardioversion can be used at any time and certainly must be used in the unstable patient. Medical cardioversion in the stable patient, or as a preventative measure in the patient who has spontaneously cardioverted will include Amiodarone or Procainamide, Procainamide may make heart failure worst in those patients with impaired left ventricular function. |
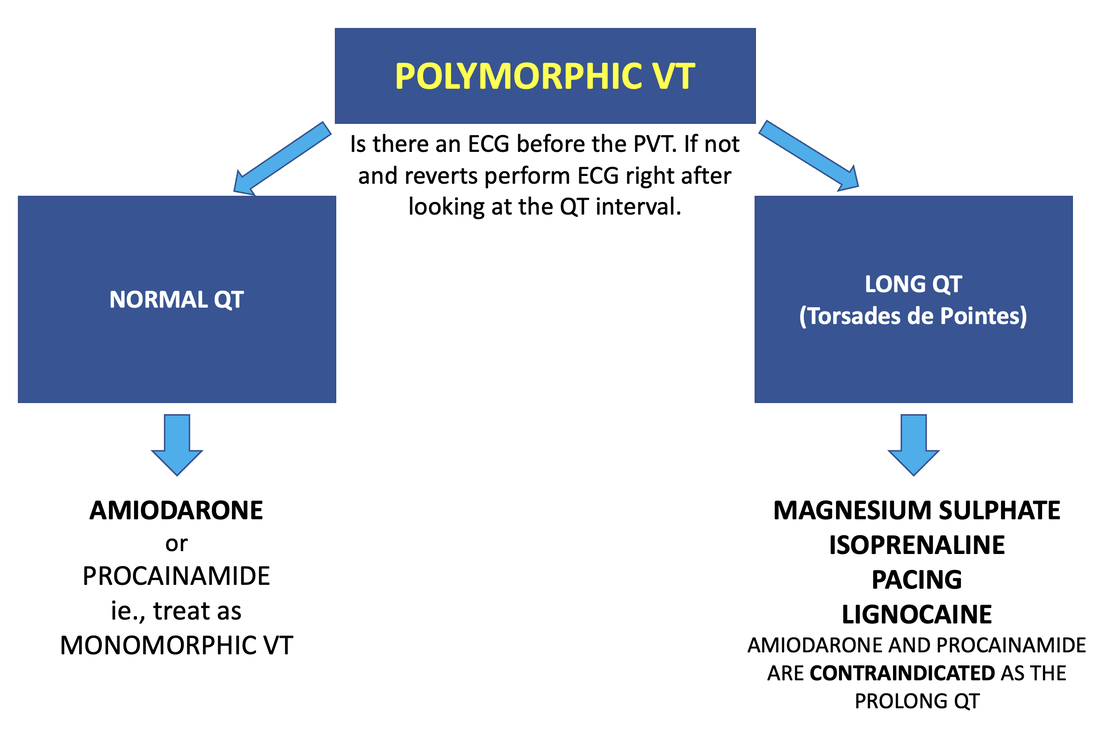
POLYMORPHIC VENTRICULAR TACHYCARDIA(PVT)
This is split into into PVT with a normal QT and that with a prolonged QT, which is known as Torsades de Pointes.
In all cases, the unstable patient should be electrically cardioverted. Stable patients can also be electrically cardioverted. In all cases of electrical cardioversion of VT, 'sync' should be used on the defibrillator.
In all cases, the unstable patient should be electrically cardioverted. Stable patients can also be electrically cardioverted. In all cases of electrical cardioversion of VT, 'sync' should be used on the defibrillator.
NOTE:
DO NOT USE
|
PVT with NORMAL QT
Causes: •Usually ischaemia •Terminates on its own •Treat it like monomorphic VT Treatment Amiodarone or Procainamide •Magnesium will probably have no effect PVT with Long QT
This is termed Torsades de Pointes It is related to prolonged QT intervals ( see ECG below) There can be congenital causes, or causes related to medications. Some medications causing prolonged QT include:
•Magnesium Sulphate IV 4g ( 16 mmol) over 1 hour •Consider Mg infusion at 4mmol/hr |
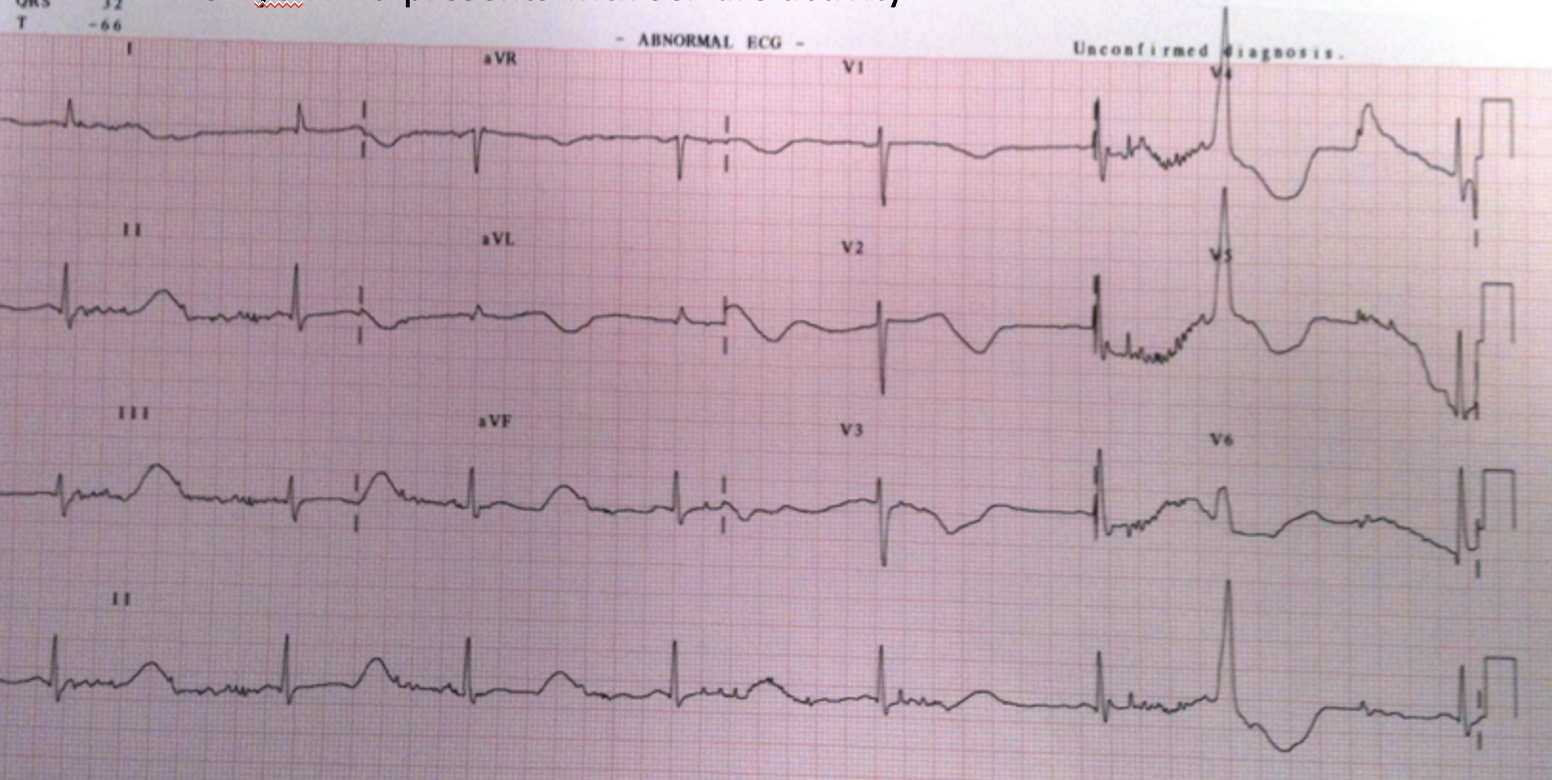
A 32 yo male patient from Methadone clinic with seizures
An ECG is done as shown below. Notice the long QT.
Soon after, the patient has a seizure and the monitor shows the strip below:
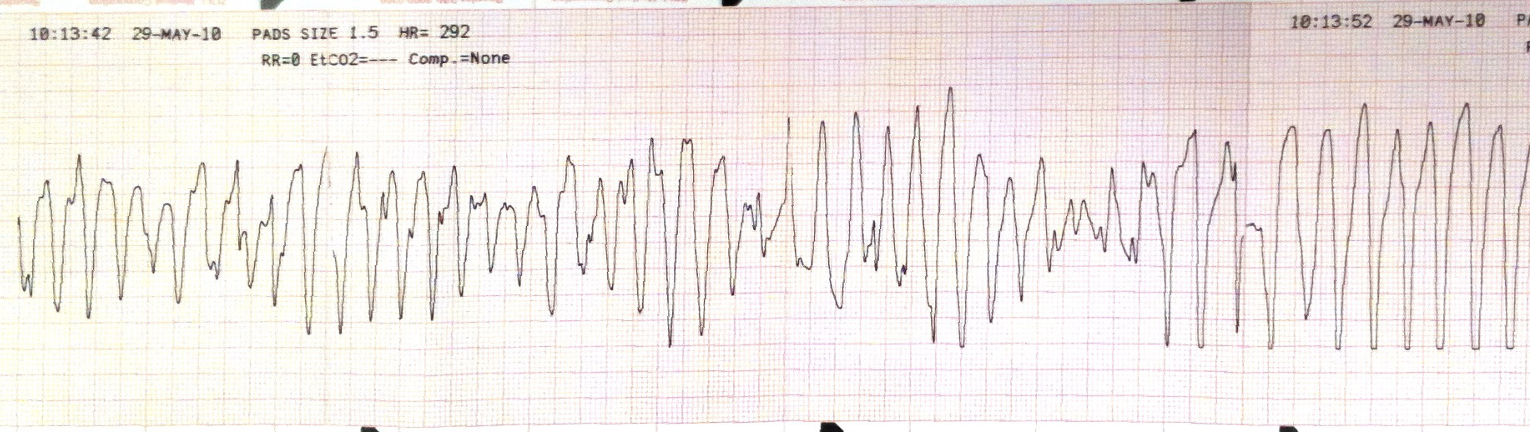
This is a Polymorphic Ventricular tachycardia. It is Torsades de Pointes as the initial ECG showed a prolonged QT interval.
The patient is shocked back into sinus rhythm and then Magnesium Sulphate is the drug to use.
DO NOT use Amiodarone or Procainamide or a Beta Blocker as they can further lengthen the QT interval.
The patient is shocked back into sinus rhythm and then Magnesium Sulphate is the drug to use.
DO NOT use Amiodarone or Procainamide or a Beta Blocker as they can further lengthen the QT interval.